Roughly 4 percent, or one in every 26, of women in America have breast implants. As the implants and surgical techniques have improved through the years, so has the desire to minimize or camouflage the incision location to maximize the aesthetic benefit of the procedure. The most common incision locations for placement of implants include: inframammary crease, in the crease below the breast, periareolar, along the lower portion of the colored portion of the areola, and transaxillary, or in the armpit.
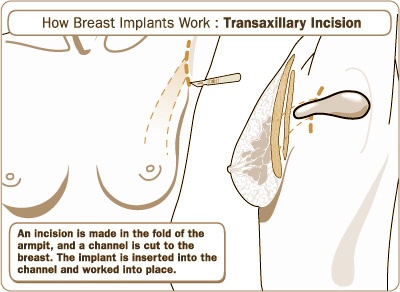
The transaxillary approach has been around since the 1970s, but it has become more popular over the last 20 years due to improved techniques and surgeon experience. The advantage of this approach is that it leaves no scars on the breast by concealing the scar in the armpit in a natural crease. The surgery can be performed by two techniques: “blind” or endoscopically assisted. Memorial Plastic Surgery prefers the endoscopically assisted technique. The advantage of using an endoscope, a lighted optical instrument with a video camera, is that the surgeon can have direct visualization of your anatomy allowing precise dissection of the pocket for placement of the implant lowering the risk for complications.
“Roughly 4 percent, or one in every 26, of women in America have breast implants”
Breast implants can be placed over the muscle, partially underneath the muscle, or completely behind the muscle/fascia with this incision. Also, both saline and silicone implants can be placed by this approach, but because silicone implants are pre-filled they may require a larger incision, greater than the standard 2.5 cm, to be placed. In addition, placement of the newer generation, anatomic-shaped silicone implants are often more difficult to insert and position properly with this approach due to their texturing and need for exact positioning.
Indications for the transaxillary approach to breast augmentation include the patient’s desire for a remote incision not on the breast, too small of an areola for placement of an incision large enough to insert an implant, and absence of a well developed crease below the breast, known as the inframammary fold, to allow a well-hidden incision when viewed in the horizontal visual field. The axillary approach has limited application in a patient who already has had breast augmentation. In addition, certain breast shapes, like tuberous breasts, may be better corrected with other access incisions.
“Over 286,000 women in America in 2014 had their breast augmented according to the American Society of Plastic Surgeons”
Complication rates for this procedure are comparable to other techniques for breast augmentation. The possible downside of using a transaxillary incision is that if a complication or need for implant replacement occurs, a new incision, often in the inframmary region, is required. The placement of implants by this technique is much easier than removal due to its remote location and limited access. As with any procedure there are risks specific to the transaxillary approach which includes implant malposition, axillary hematoma, axillary banding, and temporary swelling of lymph nodes under the arm. Axillary banding, which are fibrous bands either from lymphatic channels or thrombophlebitis known as Mondor disease, resolve over a few weeks and are managed with warm compresses, massages and anti-inflammatories. All of the potential complications of breast augmentation include: loss of nipple sensation, bleeding, infection, capsular contracture, asymmetry, unsatisfactory results, need for revisionary surgery, implant failure, implant rippling, sensory changes, and scarring.
Post-operative incision management is minimal and plastic surgeon specific. Limitations on activity level after surgery will be directed by your surgeon. Recovery time is minimal, and returning to work is often achieved in less than a week. An upper-pole strap may be necessary to wear for several days or weeks to place pressure on the implant in an inferior direction so the implants are not too high on the chest. Massage of the implant pocket is begun at two weeks.
While endoscopically assisted transaxillary augmentation has become more popular over the last 20 years, the learning curve for this technique is significant. Therefore, it is important to find a plastic surgeon certified by the American Board of Plastic Surgery who has the expertise in performing this technique.
For more information call 713.633.4411 or visit www.memorialplasticsurgery.com. Memorial Plastic Surgery is located at 929 Gessner Road, Suite 2250 in Houston, TX 77024.





Recent Comments